Introduction: The Importance of Accurate Oxygen Monitoring
Oxygen monitoring is a cornerstone of modern healthcare, critical for assessing respiratory and cardiovascular function. Yet there's ongoing confusion—even among clinicians—about the difference between PO2 and SpO2. These two measurements are related but distinct, each with unique clinical uses.
This guide will help clarify the difference, explain how each is measured, and offer practical tips for interpreting results in patient care. Whether you're a respiratory therapist, nurse, physician, or biomedical technician, understanding these concepts is essential for safe, effective monitoring.
Why It Matters: Patient Safety and Clinical Decisions
Accurate oxygen measurement guides treatment decisions ranging from supplemental oxygen administration to ventilator management. Misunderstanding these terms can lead to inappropriate interventions or missed signs of hypoxia.
For example, relying solely on SpO2 in a patient with carbon monoxide poisoning may provide false reassurance. Similarly, underappreciating a low PO2 from arterial blood gas (ABG) testing can miss significant hypoxemia even if SpO2 appears normal.
Clear communication between the care team depends on shared understanding of these metrics.
What is PO2?
PO2 stands for partial pressure of oxygen and reflects the amount of oxygen dissolved in plasma. It is measured in millimeters of mercury (mmHg) using arterial blood gas (ABG) analysis.
Key points about PO2:
- Direct measure of oxygen dissolved in blood
- Normal arterial PO2 on room air is roughly 80–100 mmHg
- Influenced by age, altitude, ventilation-perfusion matching
- Essential in assessing gas exchange and respiratory function
Clinical use: PO2 is a key indicator in diagnosing hypoxemia, assessing severity of respiratory failure, and managing mechanical ventilation settings.
What is SpO2?
SpO2 stands for peripheral capillary oxygen saturation and is measured non-invasively via pulse oximetry. It represents the percentage of hemoglobin binding sites occupied by oxygen.
Key points about SpO2:
- Quick, non-invasive, continuous monitoring
- Normal range typically 95–100% on room air
- Affected by peripheral perfusion, motion, nail polish, and sensor placement
- Less accurate at very low saturations (<80%)
Clinical use: SpO2 is widely used for real-time monitoring in settings from EMS to ICU. It's critical for titrating oxygen therapy and identifying acute desaturation events.
The Oxyhemoglobin Dissociation Curve: Bridging PO2 and SpO2
The relationship between PO2 and SpO2 is non-linear, defined by the oxyhemoglobin dissociation curve.
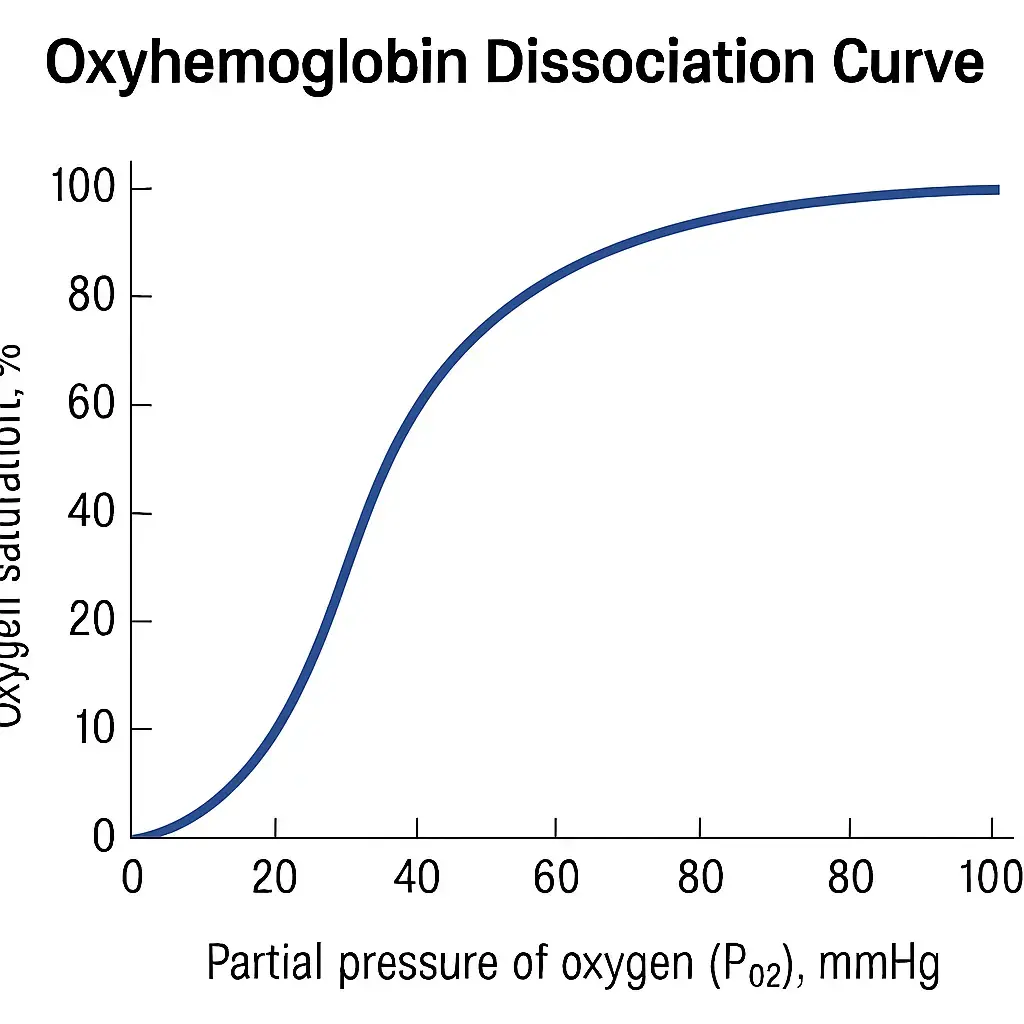
- At higher PO2 (60–100 mmHg), SpO2 plateaus at ~90–100%
- Below ~60 mmHg PO2, SpO2 drops steeply, indicating hypoxemia
Clinical insight:
- A patient with PO2 55 mmHg might have an SpO2 of ~88%
- Hypercapnia, acidosis, temperature, and 2,3-DPG levels can shift the curve
- Always interpret SpO2 in the context of patient physiology
PO2 vs SpO2: Key Differences
| Feature | PO2 | SpO2 |
|---|---|---|
| What it measures | Dissolved O2 in plasma | % of hemoglobin saturated with O2 |
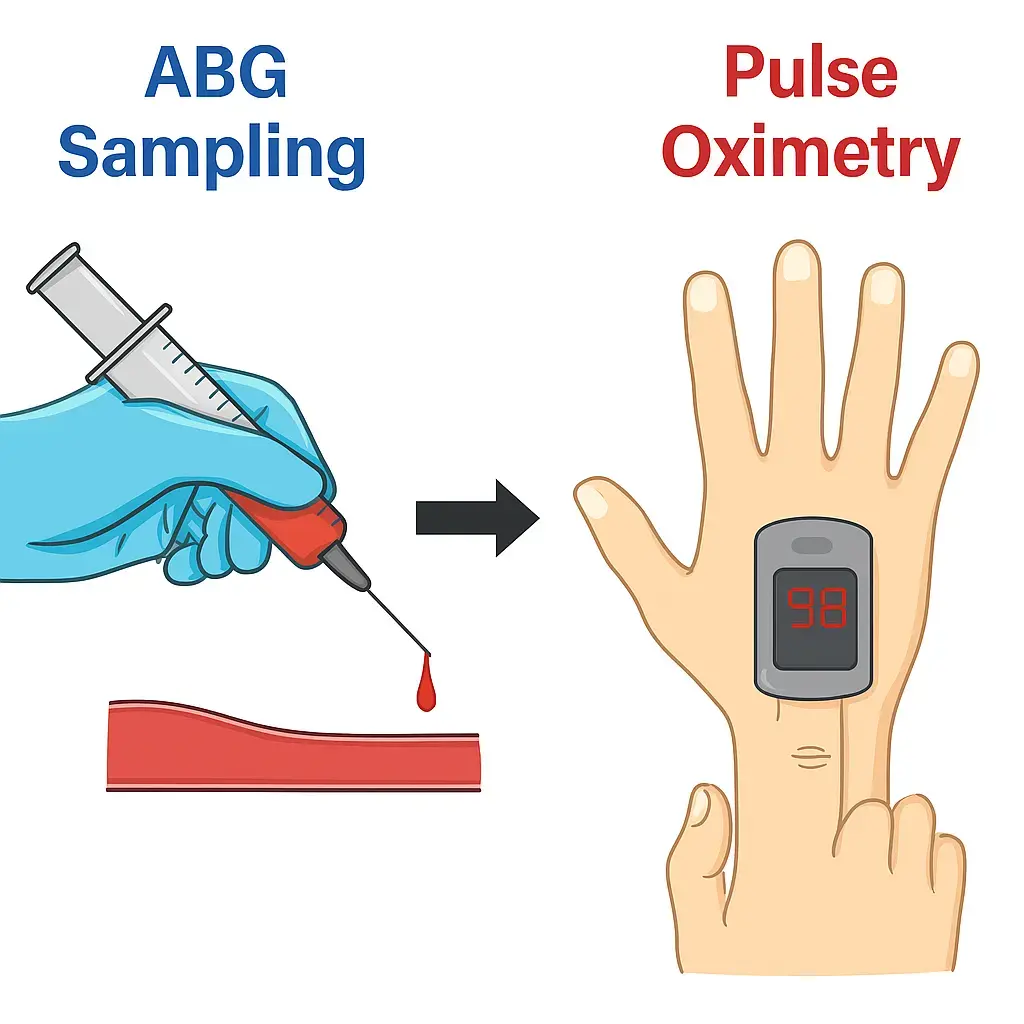
| How it's measured | Arterial blood gas (invasive) | Pulse oximeter (non-invasive) |
| Units | mmHg | % |
| Advantages | Direct, precise, diagnostic | Continuous, quick, easy |
| Limitations | Requires blood draw | Affected by motion, perfusion, dyshemoglobins |
Clinical Interpretation Tips
- Never rely solely on SpO2 when patient condition suggests hypoxemia
- Low SpO2 indicates hypoxemia but normal SpO2 does not rule it out in all scenarios (e.g., CO poisoning)
- Use PO2 to assess severity and guide therapy
- ABG provides acid-base status, ventilation (PaCO2), and oxygenation (PaO2)
- Understand patient context
- Chronic COPD patients may have lower "normal" SpO2
- Altitude and age affect PO2 baselines
- Verify suspicious readings
- If SpO2 seems inconsistent with clinical picture, get an ABG
Common Misconceptions
- "SpO2 = PO2" - False. They are related but not equivalent. PO2 is the cause; SpO2 is the effect.
- "SpO2 is always accurate" - Not always. Motion, hypoperfusion, and abnormal hemoglobins can create errors.
- "Normal SpO2 means no hypoxia" - Not in CO poisoning or methemoglobinemia. Always consider the whole patient.
Real-World Examples
- Case 1: Post-op patient with SpO2 94% but dyspnea → ABG shows PO2 55 mmHg → Start oxygen therapy
- Case 2: Fire victim with SpO2 98% → ABG shows COHb elevated → High-flow O2 needed
- Case 3: COPD patient with baseline SpO2 88% → Avoid over-oxygenation to prevent CO2 retention
How to Optimize Monitoring in Practice
- Always correlate SpO2 readings with clinical assessment
- Ensure sensors are properly placed and skin is clean
- Monitor trends rather than isolated values
- Use ABG testing when precise oxygenation status is critical
- Educate staff on limitations and correct interpretation
Medten's Compatible Pulse Oximetry Sensors
Accurate monitoring depends on reliable equipment. Medten offers a wide range of compatible pulse oximetry sensors designed for reliable signal quality across multiple patient populations and device platforms.
Our sensors undergo rigorous testing to ensure dependable performance while providing cost-effective alternatives to OEM accessories.
Frequently Asked Questions (FAQ)
Q: Is SpO2 enough for managing respiratory failure?
A: No. Always confirm with ABG to evaluate PO2, CO2, and pH.
Q: Why might SpO2 be inaccurate?
A: Motion, poor perfusion, dark nail polish, ambient light, and abnormal hemoglobins can all interfere.
Q: Can SpO2 detect CO poisoning?
A: No. Pulse oximeters can't distinguish oxyhemoglobin from carboxyhemoglobin. ABG with CO-oximetry is needed.
Q: What's a normal PO2?
A: Typically 80–100 mmHg on room air, varies with age and altitude.
Disclaimer
This content is provided for informational purposes only and does not constitute medical advice. Always follow your institution's protocols and manufacturer guidelines.